
I have worked for the NHS for the last 13 years. I have been in my current role working for a regional Integrated Care Board for the last 7 years. The Labour Party in the UK, had announced on 13th March 2025 that the government will legislate to abolish the quango, NHS England. The functions of NHS England will be integrated into the government body Department of Health and Social Care.
Integrated care boards (ICBs) answers to NHS England, which in turn answers to the Department of Health and Social care. Logic will dictate that if you cut out the ‘middle man’ -NHS England, the system should become more efficient. Messages will get to the front line of change quicker and feedback should be quicker too. Ideas and projects could be implemented faster to improve people’s healthcare. A leaner, meaner healthcare system. It is all well and good in theory, until one discovers their own job is at risk.
As of late evening, of Wednesday 19th March, NHS England had given instructions to all directors of ICBs, that ICB running costs need to be cut by 50%, by end of December 2025.
What could this mean? How will this affect ICB staff? How will this affect me? These are naturally the questions on the front of your mind, if you are an ICB employee, like me.
Here are some numbers.
There are currently 42 ICBs, spread over 7 regions of England. Scotland and Wales are not affected by this change.
The tablet below shows a breakdown of how many people are employed in each ICB.
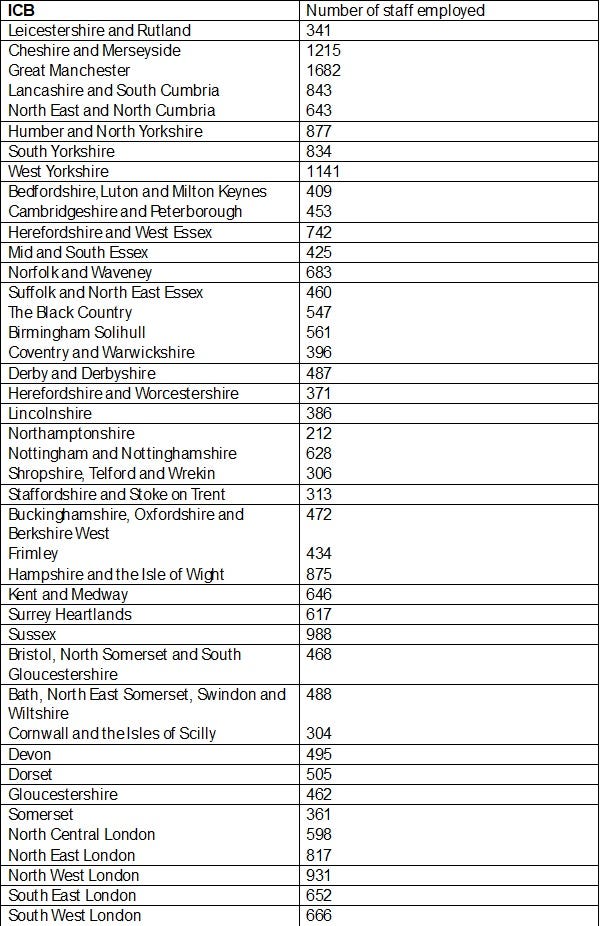

(Data obtained from ICB annual reports March 24, and article found online dated 19th September 2024. Exclusive: Highest staff cuts at Greater Manchester ICB — Healthcare Leader)
A total of 25,734 people employed by ICBs around the time March-September 2024. Perhaps some redundancies had already been made which will drive this number lower.
Some ICBs only employ administrative staff and do not provide services directly to their population of patients, whereas other ICBs employ midwives, nurses, pharmacists, technicians, consulting specialist doctors, GPs, dentists, and provide a range of clinical services.
More details of the relative numbers of administrative staff compared to healthcare staff providing services to the local population can be found by following this link: Exclusive: Admin and nursing staff make up majority of ICB workforce — Healthcare Leader
If making an assumption that 50% of jobs are to be cut, and I have found this stated in other articles online, this could mean 12,867 ICB staff could be affected by redundancies. However, there could be variation to this estimate depending on the following factors:
• Can ICBs reduce other expenses and achieve cost efficiencies elsewhere? E.g. the costs of renting premises, cost of equipment, software, services, cost of compliance. If most ICBs are renting a commercial office building, due to the nature of the commercial lease, ICBs may not be able to get out of the lease and downsize their premises, until 3–5 years later when a break in the lease is reached. Therefore, ICBs in the short term, by December 2025, may not be able to achieve any cost cuts from down-grading premises and getting more people to work from home.
• Will cost cutting be focused on highly paid Board Officers.
•Will there be jobs created elsewhere in other healthcare bodies to accommodate some of the staff displaced?
The other question that comes to my mind is that there is great variation in the number of staff and performance at each ICB. Should a high performing ICB with very few staff, be treated the same as a low performing ICB, which employs a large number of staff, and consistently under-delivers on their target measures? As in all cut by 50%?
The way forward as to how the decisions will be made, as to which functions will be lost from ICB and which divisions will be cut, is not clear at all for the moment. However, a friend of a friend who is a full-time consultant in a hospital, who also hold an adversary post designed to transform health services in a given specialty and who works around 6 hours a week for an ICB, has been dismissed from their ICB role with immediate effect and no redundancy pay.
For people, like me, who are experiencing job insecurity and possibly facing redundancy from work, I think it is best to adopt the approach ‘Hope for the best, while preparing for the worse.’
Recognising and accepting that what is happening is not within your control can be helpful. Instead of feeling anxious and staring into the uncertainty, it may be better use of your time to instead focus on the aspects of your life and actions that are within your control. I have written another article about an action plan for possible redundancy. I hope this will help others. While the person who will be made redundant might not even be you, it is still useful to go through these thought processes.
To the powers who wield the scalpel, who must make difficult decisions, as to which ICB services need to stand down and which staff members need to stand down; I beseech you to carefully consider the impact on the British population’s health. Don’t lose sight of the forest for the trees. Don’t get lost in bureaucracy and saving targets, at the cost of people’s lives and people’s suffering. Think long term. Be far sighted. Are you letting go of talented people that could contribute greatly?
Will cutting cost this year for the sake of ‘cost cutting’, actually make people’s healthcare better or worse in the long run, in the next 5 years, how about in the next 10 years?

Leave a Reply